
The “smart” revolution is transforming point-of-care devices
Diagnostic ultrasound devices, like many technologically intensive products, have undergone a dramatic change over the last 25 years. From a barely movable 500-pound cart-based platform complete with a top-mounted cathode ray tube monitor, to a hand-held “smart device” with either an attached or wireless probe, the physical nature and intended use of ultrasound devices have transformed dramatically since 1990.
The spread of ultrasound technology into point-of-care devices such as the Philips Lumify has brought cost-effective, high-quality imaging and color flow to virtually all points of the globe. But with this major technological change comes rethinking how to properly care for and test the performance of smartphone-based ultrasound devices.
Ultrasound systems have become software-centric with more generic control hardware. However, the probes themselves have become increasingly complex as front-end electronics like the beamformer (previously located in the ultrasound mainframe) have migrated to the probe. Fortunately for those who take care of ultrasound devices, the laws of physics have not changed during the last 25 years.
A new service paradigm has been evolving to accommodate this migration of ultrasound technology into an ever-increasing number of smart devices. Given that all the electronics necessary to drive a probe from a smartphone reside within the probe itself, it’s important to briefly review how transducers are constructed and how they work to set the stage for the testing and servicing discussion that follows.
Transducer Construction
The vast majority of contemporary commercially available composite multielement transducers (CMET) are composed of: 1) a piezoelectric (PZ) material that provides the necessary transduction of mechanical to electrical energy and vice versa, and 2) a supporting polymer that isolates the element while shaping the mechanical and electrical properties of the PZ elements. The physical distribution of PZ and polymer makes the array and specifies its acoustic behavior. The actual array construction is based upon well established “dicing and filling” techniques used in transducer manufacturing.
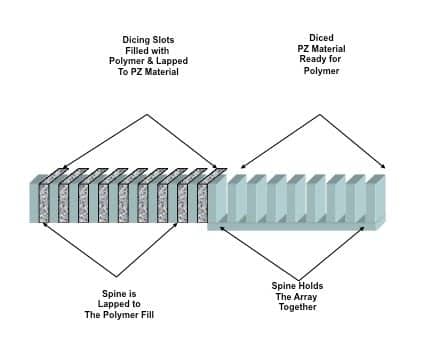
Figure 1. Acoustic array construction (click to enlarge)
Array construction begins with a block of PZ material that is “diced” to form PZ elements held by a common spine. The diced regions are then filled with polymer, as seen in Figure 1. By lapping the array “front” and “back” to remove polymer on the face and the PZ spine on the back, the manufacturer sets the array center operating frequency and sets the final configuration. The distribution of PZ and polymer provides a specific pattern of connectivity and coupling.
Connectivity refers to the continuity of each material along each of the three axes. Specific dicing and filling can produce an array that looks like a PZ-polymer sandwich (common to many current linear, convex, and phased arrays), or an array of PZ elements where each is surrounded by polymer (found in 1.5D and 2D arrays).
Coupling refers to the ability to transfer ultrasound out of an array and into the patient’s tissues and the reverse when echoes return. Acoustic coupling improves when quarter-wave layers of material with intermediate acoustic impedance values are bonded to the array face. Both connectivity and coupling can currently be tested on many ultrasound probes using commercially available probe testing devices. Multiple peer-reviewed papers have shown that as few as two dead elements in a CMET transducer can compromise the clinical efficacy of an ultrasound study, reinforcing the need to test transducers on a regular basis.1-3
Just as in earlier cart-based ultrasound systems, the transducer on the smartphone-based system creates a focused beam. By using phasing controls, the transducer moves that beam in space while dynamically focusing it at various ranges to form a more uniform B-mode image frame. The rules of focusing, such as Huygens’ principle and others, are all managed by electronic controls within the probe housing. These acoustic parameters are beyond the scope of this article, but a white paper is available to those readers who wish for more detailed information.4 Suffice to say that all of these parameters must be well defined, designed, and controlled in order to produce a diagnostic quality image and protect the smart device.
Smartphones, Tablets, and Beyond
The majority of ultrasound manufacturers targeting the smartphone market have focused on Android devices, although a recently introduced product, Clarius, works with any iOS smart device as well. These companies typically provide a list of the devices for which their ultrasound application and probe have been validated. It is important to note that once the ultrasound software is loaded onto a mobile platform and the probe is plugged in via the device’s USB port, the smartphone then becomes a finished medical device as defined by the FDA.
To that end, in February 2015, the United States Food and Drug Administration (FDA) issued a revised Guidance on Mobile Medical Applications. Included in this document is the following language: “In general, if a mobile app is intended for use in performing a medical device function (ie, for diagnosis of disease or other conditions, or the cure, mitigation, treatment, or prevention of disease) it is a medical device, regardless of the platform on which it is run.” Because the OEM has transformed the smartphone into a finished medical device, it is required to have 510(k) clearance from the FDA prior to the platform being sold in the United States.5
What the ultrasound manufacturer actually sells or rents to the clinical end user is the ultrasound software and a “smart” probe. These companies do not provide the Android device. The smartphone/tablet, via the micro USB port, supplies the probe with power to operate. The downloaded ultrasound software enables patient data entry, ultrasound display, and examination storage. Control signals operate the electronics inside the probe and export the results of the ultrasound examination from the smartphone to the cloud.
It is worth noting that all Android devices have operational quirks independent of any embedded ultrasound application. Irregularities that could impact the ultrasound examination have to do with battery charge levels during use, data transfer crashes that occur during either transmit or receive, and other issues that should be researched and documented by the end user—prior to installation of the ultrasound software. This should allow the healthcare technology manager (HTM) to differentiate a problem with the ultrasound application from the normal/abnormal behavior of the core smart device.
Another performance issue that may arise when these devices are used in the hospital is electromagnetic interference (EMI), which can layer noise and other anomalous signals on the ultrasound image. The HTM should confirm potential EMI “hot-spots” in the hospital and inform the clinical user as to what he or she might expect when using the device in these areas.
Testing probes on these new mobile devices requires the same diligence necessary for probes on cart-based systems, since the intended use and expected outcome of both devices is to create a clinically efficacious image. To that end, benchmarking the clinical performance of a new device will establish a threshold against which periodic quality assurance (QA) testing can be measured.
When thinking about maintenance strategies for these device always remember, failures tend to cluster around the weakest points of the device’s design. For example, USB connectors and cables are often a source of problems due to their fairly delicate design, so rule out these first when troubleshooting a malfunction, and have a couple of extra connectors and cables on your desk. There is also the possibility that a problem within the probe could significantly damage the Android device—for instance, a high-voltage short sparking a low-voltage line feeding back to the device. If you see a “puff of smoke” coming from your Android device while using the probe, it might be a hint to discontinue use.
The Future is Sound
Although the diffusion of ultrasound technology to commercial off-the-shelf devices will continue to grow rapidly, they are still very basic modality devices with a limited feature set. The more eclectic yet important modalities such as 3D volumetric imaging, shear wave elastography, and strain gauge imaging—all requiring significant processing capacity—remain the domain of cart-based ultrasound systems, and will for the foreseeable future.
But the architecture of cart-based systems has changed from a proprietary, hardware-centric structure to a software-centric (eg, Windows-embedded standard 2009), specialized front-end and generalized back-end structure. Due to their software-centric structure, the newer cart-based devices experience system failures associated with the software and hard drives at a much higher rate than those due to the core operation ultrasound hardware. During the last 10 years, more than 85% of all ultrasound system recalls were related to software.6 Therefore, the key to maintaining these devices is to be very knowledgeable about Windows operating systems (and their quirks), and to back up everything possible on the system related to software and presets, as well as ghosting the hard drives and keeping up to date on product recalls.
Obviously, there are still hardware failures with these newer devices. They tend to cluster around design-related issues (such as pushing the performance limit of a component) or modules that heat up (like power supplies) or switch fast (for example, a beamformer). High-end, cart-based systems more frequently use complex 2D matrix array transducers for various clinical applications to view the anatomy in a volumetric manner. Although complex, these probes can (and should) be tested and performance-verified on a regular basis by the hospital HTM personnel.
Assuming Moore’s law (Gordon, not Wayne) will continue, many of these higher technology features and modes of operation will migrate to mobile devices over time. Newer and ever more complex transducers and ultrasound processing technologies will also be discovered, breathing continued life into cart-based systems. But thankfully, they will never again weigh 500 pounds.
Servicing Perspectives
What do all of these technology changes mean for servicing and maintaining these devices? The HTM team must continue to develop skills related to servicing commercial off-the-shelf devices that are being transformed into medical devices, with a strong emphasis on software, software communications, and control techniques.
Read the FDA guidance documents controlling these mobile devices. It will inform what testing you may want to integrate into your servicing armamentarium. Develop a keen understanding of the signals (both control and diagnostic data) being transmitted and received between the smart probes and the hand-held devices to determine which component may be the problem if a failure occurs. Develop and keep a service history folder on each device and document any and all quirks associated with a given hand-held device. Establish a baseline of performance when the device first comes into your facility, and document this as well. Research and implement new ultrasound test devices on the market that provide information on the proper acoustic energy output of the probe, especially with wireless probes. And buy a few extra USB connectors—they will come in handy when troubleshooting.
The diffusion of ultrasound technology into mobile devices such as smartphones increases the availability of affordable, quality ultrasound imaging performance for point-of-care applications on a global, and often underserved, basis. Ultrasound probes, too, will continue to get smarter and less expensive as new piezo materials replace current 1-3 composite arrays. Wireless performance levels will eventually reach a point that eliminates the need for a transducer cable on both cart-based and hand-held units.
As compelling as this new paradigm is, we must always keep in mind that these mobile devices are transformed into finished medical devices that must be properly maintained to ensure both the quality of clinical images and the safety of the device. By understanding the particulars of any given probe design, as well as documenting the operational quirks of the mobile device being used, we can develop and implement a rational QA and preventive maintenance program.
The shift from hardware-centric to software-centric systems means retooling not only our test device arsenal, but our thinking and equipment maintenance strategies.
Wayne Moore is CEO of Acertara Acoustic Laboratories. For more information, contact chief editor Jenny Lower at [email protected].
References
1. The Effect of Dead Elements on the Accuracy of Doppler Ultrasound Measurements, Jaromir Vachutka, Ladislav Dolezal, et al. Ultrasonic Imaging 2014, Vol 36(I) 18-34, Sage Publishing.
2. High Incidence of Defective Ultrasound Transducers in Use in Routine Clinical Practice, Martensson M, Olsson, M, et al. European Journal of Echocardiography, 2009;10:389-94.
3. The Methods and Effects of Transducer Degradation on Image Quality and the Clinical Efficacy of Diagnostic Sonography, Weigang B, Moore GW, et al. Journal of Diagnostic Medical Sonography 2003; 19: 3-13
4. The Silent Revolution: Catching Up with the Contemporary Composite Transducer, Raymond Powis, PhD, FAIUM and G. Wayne Moore, B.Sc., MA, FASE, Acertara Acoustic Laboratories.
5. Mobile Medical Applications, Guidance for Industry, Center for Devices and Radiological Health, US Food and Drug Administration, Document issued on Feb 9, 2015. http://www.fda.gov/downloads/MedicalDevices/…/UCM263366.pdf
6. http://www.fda.gov/MedicalDevices/Safety/ListofRecalls/ucm435537.htm, US Food and Drug Administration.
Lead photo caption: The Philips Lumify ultrasound device was introduced in 2015.



I love the clarity of the Philips echo images, however the machine cannot really do full echo as it lacks continuous wave and pulse wave doppler which the original advertising said that it would have. It doesn’t, a really limitation to any sort of serious echo. It’s OK for seeing pericardial effusion or tamponade, for seeing color flow in a limited way. Basic images of the heart are good. There are no color maps. On using the algorithm for ” obstetric” there were no equations to determine fetal heart rate in m-mode and nothing for fetal age estimation. Another disappointment. So far the device is sort of an elaborate toy with a lot of limitations
Where can I buy one? How much does it cost?